Aortic Shape Space Geometry

- Current clinical paradigm reduces aortic geometry to a single size quantity, the maximum diameter.
- Size alone is insufficient to capture the complex shape changes in aortic disease progression.
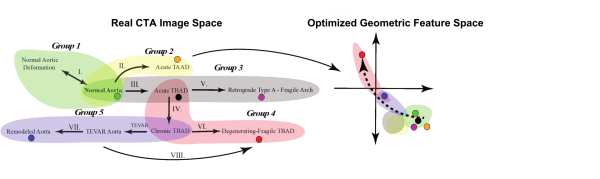
- We have identified a shape parameter, fluctuations in total curvature (δK), that can distinguish between shape preserving growth in normal aortas (1-3) and rapidly fluctuating shapes that are the hallmark of disease (4-8).
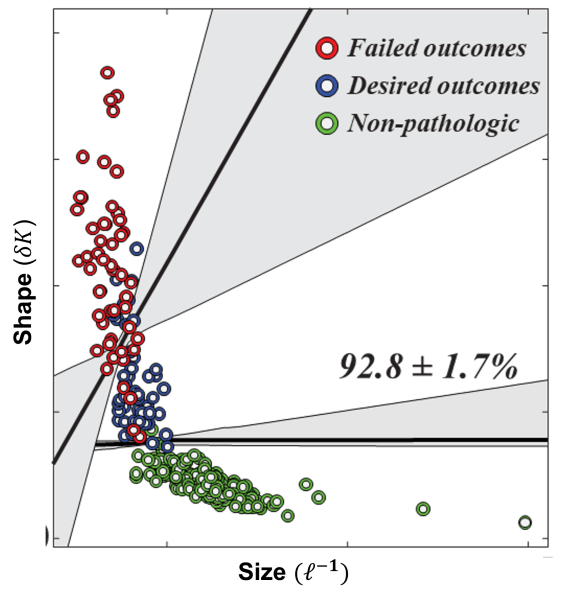
- Using a cohort of patients without aortic pathology, a cohort of TEVAR patients, and machine learning methods, δK was able to distinguish patients without aortic pathology, patients with TEVAR who had positive outcomes, and patients with TEVAR who had failed outcomes with over 92% accuracy.
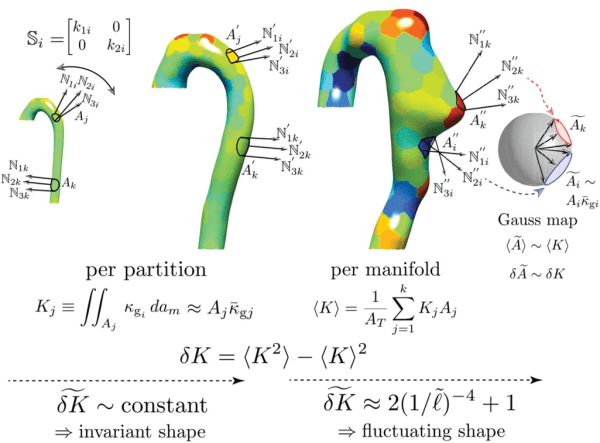
- We map the aortic surface to a unit sphere to obtain independent measures of shape using surface normals (N_i ).
- Gradients in N_i give the per-vertex principal curvatures and the per-vertex shape operator (S_i ) is calculated using the Rusinkiewicz algorithm [IEEE 3DPVT 2004].
- To minimize noise, the aorta is partitioned to calculate the local integrated Gaussian curvature defined as the product of the partition’s area and mean Gaussian curvature, K_j=A_j κ ̅gj.
- K_j is equivalent to the signed partition area, A ̃j, mapped out by the normals projected onto the unit sphere.
K_j and A ̃j are topologic invariants. We define aortic shape by studying the statistics of the first and second distribution moments of K_j,⟨K⟩ and δK, respectively.